Ortho Fracture Series 1: Proximal Humerus Fracture
The new Ortho Fracture Series will cover the most important type of fractures. It is a compilation of info from various websites and textbook.
In our very first series, we will look into proximal humerus fracture. It comprise of 4-6% of all fractures and the third most common fracture in elderly with females having higher incidence (2:1 ratio). Increasing age is also a risk factor for women.










In our very first series, we will look into proximal humerus fracture. It comprise of 4-6% of all fractures and the third most common fracture in elderly with females having higher incidence (2:1 ratio). Increasing age is also a risk factor for women.
Understanding anatomy

The 5 most important parts of proximal humerus:
- Greater tuberosity
- Lesser tuberosity
- Humeral head
- Anatomical neck (the epiphyseal plate) - located distal to the head of the humerus, at an oblique angle to the shaft of the humerus (fracture here,although rare, may lead to avascular necrosis)
- Surgical neck - most frequently fractured site of the proximal humerus (so surgeon operate here more often, hence the name, surgical neck), putting the axillary nerve and posterior circumflex humeral branch of the axillary artery at risk.

Muscle around proximal humerus
- Rotator cuff muscles: Supraspinatus, Infraspinatus, Teres Minor, (these 3 are inserted at greater tubercle) Subscapularis muscles (inserted at lesser tubercle)
- Deltoid muscle
- 3 muscles attached to bicipital groove with mnemonic ‘the lady between two majors’
Lateral to medial:
1. Pectoralis major muscle
2. Latissimus dorsi (the lady)
3. Teres major
Source: https://goo.gl/nCLhdu
Source: https://goo.gl/5kyEoY
Source: https://goo.gl/nCLhdu
Blood supply

- Axillary artery
- Posterior humeral circumflex artery
- Anterior humeral circumflex artery
- Lateral ascending branch of anterior circumflex artery- carries the MOST blood supply to humeral head, its damage --> avascular necrosis (AVN) of humeral head, thus is location is vital for classification and prognosis, vascularity-sparing dissection, and implant placement (see * below)
- Greater tubercle
- Lessed tubercle
- Tendon insertion of infraspinatus muscle
- Tendon insertion of teres minor muscle
Also note that the medial aspect of capsule has the second most blood supply. It is supplied by metaphyseal vessels and vessels of greater and lesser tuberosities that anastomose with the intraosseous arcuate artery. The sparing of this part will have a better prognosis.
# Fracture at the anatomical neck with a medial metaphyseal (calcar) spike shorter than 8mm carry high risk of AVN of humeral head.
# Fracture at the anatomical neck with a medial metaphyseal (calcar) spike shorter than 8mm carry high risk of AVN of humeral head.
*Tendon of long head of bicep brachii plays an important to localize position of lateral ascending branch of anterior circumflex artery and to orientate greater and lesser tubercle.

In fractures that could not be reduced via closed reduction, the bicep tendon may be trapped between bone fragment. The acromion, coracoacromial ligament, and coracoid process form an arch under which the humeral head rotates. Humeral head movement is constrained by this arch, while the muscles of the rotator cuff guide movement under the arch.
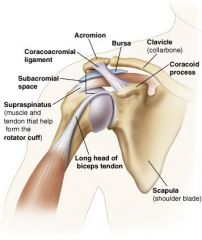
Source: http://fce-study.netdna-ssl.com/2/images/upload-flashcards/89/79/11/9897911_m.jpg
Pathophysiology of Proximal Humerus Fracture
Classification
The most commonly used classification is Neer classification, which is based on X ray appearances, where the injuries. This system divides proximal humerus into 4 segments: greater tuberosity, lesser tuberosity, head of humerus and the humeral shaft. It takes into account displacement and not the number of fracture line, with displacement >45 degrees of angulation or 1cm of separation. So, take note: no matter how many fracture lines there are, if it is not displaced, it is considered as one-part fracture.




Refer here for more info.
Clinical features



Fracture-dislocation- Low energy fall: in case osteoporotic bones (eg: fall on outstretched hand)
- High energy trauma: young people, may have shoulder dislocation too
- Others: from violent muscle contractions (seizure, activity, electrical shock, and athletic injuries), direct blow to proximal humerus
Classification
The most commonly used classification is Neer classification, which is based on X ray appearances, where the injuries. This system divides proximal humerus into 4 segments: greater tuberosity, lesser tuberosity, head of humerus and the humeral shaft. It takes into account displacement and not the number of fracture line, with displacement >45 degrees of angulation or 1cm of separation. So, take note: no matter how many fracture lines there are, if it is not displaced, it is considered as one-part fracture.

One-part fracture from AP and lateral radiograph of proximal humerus
Two-part fracture involving the surgical neck
Refer here for more info.
Clinical features
- Look for large bruise on upper part of arm
- Pain is less severe because the fracture is often firmly impacted
- Signs of axillary nerve injury: reduction in shoulder abduction (as it supplies the deltoid muscle), weakness in flexion and external rotation, dull, aching pain at deep/lateral shoulder with or without radiation to proximal arm, which increases with range of motion, fatigue, especially with overhead activities, heavy lifting, and/or throwing
- History of trauma/dislocation
- Sign of brachial plexus injury

Source: https://goo.gl/NcY8mr
Loss of sensation at regimental badge area
Source: https://goo.gl/v89wWE

Source: UCLA health https://goo.gl/PTfYi7
Treatment
Minimally displaced fracture
- Non-operative
- 1-2 weeks of rest
- Arm sling till pain subsides
- Gentle passive movements of shoulder, exercise from elbow and below are allowed and highly encouraged
- Encourage active exercises after union (usually after 6 weeks)
Two-part fracture
1. Surgical neck fractures
Conservative measures (generally works as elderly patient do not demand for perfect function)
1. Surgical neck fractures
Conservative measures (generally works as elderly patient do not demand for perfect function)
- closed reduction
- immobilized arm in a sling for about 4 weeks or until fracture is stable and x-ray shows signs of healing
- encourage elbow and hand exercises
- Start shoulder exercise at about 4 weeks
Operative measures
- if fracture cannot be reduced close or fracture is unstable post-close reduction
- Options includes: Percutaneous pins, bone sutures, intramedullary pins with tension band wiring or a locked intramedullary nail
2. Greater tuberosity fractures
- often associated with anterior dislocation of shoulder, hence it realign well when shoulder is relocated
- If not, the fragment can be reattached through a small incision with intraosseous sutures or, in young hard bone, cancellous screw.
3. Anatomical neck fractures
- very rare
- young patients: fix with screw
- older patients: prosthetic replacement (hemiarthroplasty) - due to high risk of avascular necrosis of the humeral head
Three-part Fractures
- usually involve displacement of surgical neck and greater tuberosity
- difficult to reduce closed
- Active individuals: Open reduction, internal fixation (ORIF)
- Osteoporotic bone: Implants + locked plating and nailing
Four-part Fractures
- High risk of complications: Vascular injury, brachial plexus damage, injuries to chest wall and avascular necrosis of humeral head
- Difficult x-ray diagnosis
- Young patient: Reconstruction and internal fixation
- Older patient: Hemiarthroplasty (as we are afraid of continuing pain and stiffness, and compromising blood supply). However, the result is unpredictable. It depends on anatomical reduction, fixation and healing of tuberosities
- Two-part fracture-dislocations (greater tuberosity + anterior dislocation of shoulder and lesser tuberosity + posterior dislocation of shoulder) can be reduced closed
- Three-part fracture dislocation (with surgical neck also broken): ORIF (brachial plexus will be at risk)
- Four-part fracture dislocation: poor prognosis, prosthetic replacement is preferred in all except young, very active patients.
Complications
- AVN of humeral head: 10-30% in 3-part #, 10-50% in 4-part #
- Shoulder stiffness - common especially in elderly, it can be prevented/minimized with early exercises
- Malunion: usually causes little disability, but loss of rotation may make it difficult for patient to reach behind the neck or up the back
In children
1. At birth
- shoulder is sometimes dislocated or present of proximal humerus
- difficult to diagnose
- look for clavicular fracture or brachial plexus injury
2. In infancy
- the physis can separate (Salter-Harris I)
- Reduction does not have to be perfect
- Usually has good outcome
3. Older children
- metaphyseal fractures / Type II physeal fractures occur
- considerable displacement and angulation can be accepted
- malunion is readily compensated due to the remodelling potential and marked growth
- Pathological fracture is NOT uncommon as proximal humerus is the site of bone cysts and tumours in children
- Fracture through a simple cyst usually unites and the cyst usually heals spontaneously
- Treatment: Rest arm in a sling for 4-6 weeks
Hope it will be useful in some ways. :D
Good day to all
Signing out,
J & Fi
References:
1. TeachMeAnatomy
2. AO Foundation: https://goo.gl/yagsQo
3. https://goo.gl/yY53mf
4. https://goo.gl/Vg0dVq
5. https://goo.gl/5kyEoY
6. Orthobullets: https://goo.gl/x7opVk
7. Medscape Proximal Humerus Fracture: https://goo.gl/hnhVDC
8. Apley's Systems of Orthopedics and Fractures Textbook, 9th edition page 744-747
9. Radiopedia: https://goo.gl/SqIhfF
10. Physiopedia - Axillary Nerve Injury: https://goo.gl/NcY8mr
11. UCLA health - Brachial Plexus Injury https://goo.gl/PTfYi7


Comments
Post a Comment